[1] J.E. Ballard, R.A. Boileau, E.K. Sleator, B.H. Massey and R.L. Sprague, "Cardiovascular responses of hyperactive children to methylphenidate."
JAMA (1976) Dec 20;236(25):2870-4.
[2] F.K. Blatchford, R.G.Knowlton, and D.A. Schneider (1985) "Plasma FFA responses to prolonged walking in untrained men and women,"
European Journal of Applied Physiology (1985), Vol. 53, pp. 343-347.
[3] P. R. Breggin, M.D.,
Talking Back to Ritalin: What Doctors aren't Telling you about Stimulants and ADHD , revised edition, Da Capo Press, Cambridge, MA, 2001.
[4] J.R. Burgess et al., "Essential fatty acid metabolism in boys with attention deficit-hyperactivity disorder,"
American Journal of Clinical Nutrition 1995; 62, pp. 761-68.
[5] F.X. Castellanos et al., "Developmental trajectories of brain volume abnormalities in children and adolescents with attention deficit hyperactivity disorder,"
JAMA (2002), Vol. 288, NO. 14, pp. 1740--1748.
[6] J. C. Chatham, "Lactate: The Forgotten Fuel,"
J. Physiol. (2002) Vol 542(2), p. 333.
[7] Jorge Chavarro, Walter C. Willett, and Patrick J. Skerrett,
The Fertility Diet, McGraw Hill, 2008.
[8] D. Coghill and T. Banaschewski, "The genetics of attention-deficit/hyperactivity disorder,"
Expert Rev Neurother (2009) Oct, Vol. 9 No. 10, pp. 1547-65.
[9] B. Garcia, Y. Wei, J.A. Moron, R.Z. Lin, J.A. Javitch and A. Galli, "AKT is essential for insulin modulation of amphetamine- induced human dopamine transporter cell surface redistribution,"
Molecular Pharmacology (2005); DOI: 10.1124/mol.104.009092
[10] E.R. Garwood, W. Bekele, C.E. McCulloch and C.W. Christine, "Amphetamine Exposure is Elevated in Parkinson's Disease,"
NeuroToxicology, Vol. 27, No. 6, December 2006, Pages 1003-1006.
[11] Barry Groves,
Trick and Treat: How 'Healthy Eating' is Making us Ill, Hammersmith Press, 2008.
[12] M. Guzmán and C. Blázquez, "Ketone body synthesis in the brain: possible neuroprotective effects."
Prostaglandins Leukot Essent Fatty Acids (2004) Mar, Vol. 70, No. 3, pp. 287-92.
[13] E. Heininger, "A unifying hypothesis of Alzheimer's disease. IV. Causation and sequence of events,"
Rev Neurosci. (2000) Vol. 11 Spec No:213-328.
[14] S. Holmberg, A. Thelin and E.-L. Stiernström, "Food Choices and Coronary Heart Disease: A Population Based Cohort Study of Rural Swedish Men with 12 Years of Follow-up,"
Int. J. Environ. Res. Public Health (2009) Vol. 6, pp. 2626-2638; doi:10.3390/ijerph6102626.
[15] G. Hornstra, "Essential fatty acids in mothers and their neonates,"
Am. J. Clin Nutr. (2000) Vol 71 (5 suppl), pp. 1262S-1269S.
[16] M. Kinsbourne, "Sugar and the hyperactive child,"
New England Journal of Medicine, (1994) Feb 3, pp. 355-356.
[17] A. F. La Berge, "How the Ideology of Low Fat Conquered America,"
Journal of the History of Medicine and Allied Sciences, (2008) Feb. 23, Vol. 63, No. 2, pp. 139-177; doi:10.1093/jhmas/jrn001
[18] N. Lambert and C.S. Hartsough, "Prospective study of tobacco smoking and substance dependence among samples of ADHD and non-ADHD subjects,
Journal of Learning Disabilities (1998) Vol. 31, pp. 533-534.
[19] L. Langseth and J. Dowd, "Glucose tolerance and hyperkinesis," (1978)
Food Cosmet. Toxicol. Vol. 16, p. 129.
[20] J.C. McCann and B.M.Ames BN, "Review Article: Is there convincing biological or behavioral evidence linking vitamin D deficiency to brain dysfunction,"
FASEB J. (2008) Vol. 22, pp. 982-1001.
[21] D. Modan-Moses, D. Stein, C. Pariente, A. Yaroslavsky, A. Ram, M. Faigin, R. Loewenthal, E. Yissachar, R. Hemi, and H. Kanety, "Modulation of Adiponectin and Leptin during Refeeding of Female Anorexia Nervosa Patients,"
The Journal of Clinical Endocrinology & Metabolism, Vol. 92, No. 5, pp. 1843-1847.
[22] S.H. Mostofsky, A.L. Reiss, P. Lockhart and M.B. Denckia, "Evaluation of cerbellar size in attention deficit-hyperactivity disorder,"
Arch. Gen. Psychiatry, (1996) Vol. 53, No. 7, pp. 607--616.
[23] V. Mougios, S. Ring, A. Petridou, and M.G. Nikolaidis, "Duration of coffee- and exercise-induced changes in the fatty acid profile of human serum,"
J Appl Physiol (2003) Vol. 94, pp. 476-484. doi:10.1152/japplphysiol.00624.2002
[24] H. Okuda, Y. Saito, N. Matsuoka and S. Fujii, "Mechanism of Adrenaline-induced Lipolysis in Adipose Tissue,"
J. Biochem, (1974) Vol. 75, No. 1, pp. 131-137.
[25] F. Ottoboni, M.P.H., Ph.D, and A. Ottoboni, Ph.D., "Can Attention Deficit-Hyperactivity Disorder Result from Nutritional Deficiency?",
J. American Physicians and Surgeons, Vol. 8, No. 2, Summer, 2003.
[26] W.A. Price,
Nutrition and Physical Degeneration, Los Angeles, Calif., Keats Publishing ;1998 (First Edition, 1939).
[27] B. Quistorff, N.H. Secher and J.J. Van Lieshouts, "Lactate fuels the human brain during exercise",
The FASEB Journal (2008), Vol. 22, pp. 3443-3449. doi: 10.1096/fj.08-106104.
[28] U. Ravnskov, M.D., PhD,
Fat and Cholesterol are Good For You,, G. B. Publishing, Sweden, 2009.
[29] A. Richardson and B. Puri, "Randomized double-blind, placebo-controlled study of the effects of supplementation with highly unsaturated fatty acids on ADHD-related symptoms in children with specific learning difficulties,"
Prog Neuropsychopharmacol Biol Psychiatry, Vol 26(2), 2002, pp. 233-9.
[30] R.A. Robergs, and S.O. Roberts,
Exercise Physiology: Exercise, Performance, & Clinical Applications, (1997) WCB McGraw-Hill, Boston, MA.
[31] P. Shaw, K. Eckstrand,W. Sharp, J. Blumenthal, J.P. Lerch, D. Greenstein, L. Clasen, A. Evans,J. Giedd and J.L. Rapoport, "Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation",
Proceedings, National Academy of Sciences (2007) December 4,, Vol. 104, No. 49, pp. 19649-19654.
[32] Silver L.B. Attention-Deficit Hyperactivity disorder. Clinical guide to diagnosis and treatment. Washington: American Psychiatric Press Inc, 1992: 129-134.
[33] N. Sinn, "Physical fatty acid deficiency signs in children with ADHD symptoms,"
Prostaglandins Leukot Essent Fatty Acids (2007) Aug; Vol. 77 No. 2, pp. 109-15. Epub 2007 Sep 6.
[34] L.J. Stevens et al. "Essential fatty acid metabolism in boys with attention-deficit hyperactivity disorder,"
Am J Clin Nutr (1995) Vol. 26, No. 8, pp. 406--411.
[35] Gary Taubes,
Good Calories Bad Calories:Challenging the Conventional Wisdom on Diet, Weight Control, and Disease.,
Alfred A. Knopf., 2007.
[36] N.D. Volkow, G.J. Wang, S.H. Kollins, T.L. Wigal, J.H. Newcorn, F. Telang, J.s. Fowler, W. Zhu, J. Logan, Y. Ma, K. Pradhan, C. Wong, and J.M. Swanson, "Evaluating dopamine reward pathway in ADHD: clinical implications."
JAMA (2009) Sep 9; Vol. 302, No. 10, pp. 1084-91.
[37] N.D. Volkow, Y.-S. Ding, J.S. Fowler, G.-J. Wang, J. Logan, J.S. Gatley, S. Dewey, C. Ashby, J. Lieberman, R. Hitzemann and A.P Wolf, "Is methlphenidate like cocaine?"
Archives of General Psychiatry, (1995) Vol. 52, pp. 456--463.
[38] I.T, Yamamoto and M. Sugano, "Effect of dietary fat on lipid secretion and ketone body production in rat liver,"
J Nutr Sci Vitaminol> (Tokyo) (1984) Apr, Vol. 30 No. 2, pp. 153-62.
 autism in America may also be attributable to maternal deficiencies in these key nutrients, especially when the pregnant mother is sufficiently disciplined to remain thin despite strong temptations to eat. In this essay, I will develop a theory that Attention Deficit Hyperactivity Disorder (ADHD), a disease that barely existed before the 1970's, but is now steadily increasing in incidence rates in the United States, is also likely caused by inadequate dietary fats, with a possible contributory role played by vitamin D deficiency.
autism in America may also be attributable to maternal deficiencies in these key nutrients, especially when the pregnant mother is sufficiently disciplined to remain thin despite strong temptations to eat. In this essay, I will develop a theory that Attention Deficit Hyperactivity Disorder (ADHD), a disease that barely existed before the 1970's, but is now steadily increasing in incidence rates in the United States, is also likely caused by inadequate dietary fats, with a possible contributory role played by vitamin D deficiency. Today it is practically impossible to find full-fat yogurt at an American grocery store, and non-fat or low-fat products crowd out the full-fat versions of the same things on grocery shelves. Marketing ploys are proud to boast that a given product contains little, or, better yet, no, fat.
Today it is practically impossible to find full-fat yogurt at an American grocery store, and non-fat or low-fat products crowd out the full-fat versions of the same things on grocery shelves. Marketing ploys are proud to boast that a given product contains little, or, better yet, no, fat. supplement have shown modest but encouraging results. However, I'm not proposing simply adding an omega-3 pill alongside the Ritalin tablet. I'm proposing that the cheerios and skim milk for breakfast be replaced with bacon and eggs; that the diet coke for lunch be replaced with whole milk, and the lean turkey breast in the sandwich be replaced with dark tuna, peanut butter, or liverwurst (a healthy choice that has all but disappeared from America's grocery shelves).
supplement have shown modest but encouraging results. However, I'm not proposing simply adding an omega-3 pill alongside the Ritalin tablet. I'm proposing that the cheerios and skim milk for breakfast be replaced with bacon and eggs; that the diet coke for lunch be replaced with whole milk, and the lean turkey breast in the sandwich be replaced with dark tuna, peanut butter, or liverwurst (a healthy choice that has all but disappeared from America's grocery shelves). against ADHD because the abundant fat cells can release plenty of triglycerides into the blood early in the morning, before the first meal. This fat supply can tide the person over through the long fatty-acid drought that occurs during the day, while an abundance of high-glycemic index low-fat foods are consumed. A further advantage is that obese people typically have reduced insulin production (due to insufficient calcium, which I explain later), so the levels of insulin in the blood are never excessively high. Their muscle cells have been programmed to prefer fat metabolism, but there is also plenty of fat available from the triglycerides (released before the meal began) to supply the brain's raw materials to enhance communication through neural pathways. Furthermore, the glucose that is not consumed by the muscles is readily available
against ADHD because the abundant fat cells can release plenty of triglycerides into the blood early in the morning, before the first meal. This fat supply can tide the person over through the long fatty-acid drought that occurs during the day, while an abundance of high-glycemic index low-fat foods are consumed. A further advantage is that obese people typically have reduced insulin production (due to insufficient calcium, which I explain later), so the levels of insulin in the blood are never excessively high. Their muscle cells have been programmed to prefer fat metabolism, but there is also plenty of fat available from the triglycerides (released before the meal began) to supply the brain's raw materials to enhance communication through neural pathways. Furthermore, the glucose that is not consumed by the muscles is readily available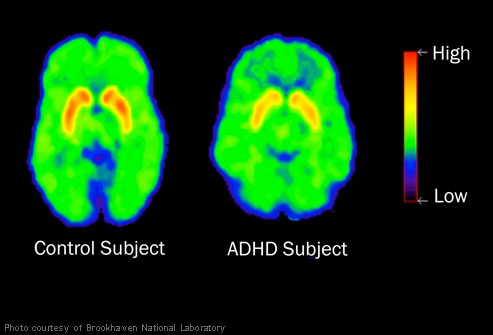
 White matter consists of a massively interconnected network of nerve fibers, each of which is coated with a fatty myelin sheath that keeps the message insulated (i.e, keeps the signal strong) and greatly increases the transmission speed. In order to focus attention, the brain releases the hormone dopamine from centers in the midbrain, and dopamine receptors transmit signals over long distance pathways to the frontal cortex, the basal ganglia, and the cerebellum, as shown in the figure on the left. Dopamine is a crucial hormone that orchestrates the brain's thought processes involved in maintaining attention to a task and subsequently acquiring new knowledge. Defective dopamine utilization is widely suspected to play a role in ADHD [36]. Poor quality white matter on these long-distance connections, as a consequence of insufficient supply of fat from the blood, would have a huge impact on the ability to pay attention and to learn new facts.
White matter consists of a massively interconnected network of nerve fibers, each of which is coated with a fatty myelin sheath that keeps the message insulated (i.e, keeps the signal strong) and greatly increases the transmission speed. In order to focus attention, the brain releases the hormone dopamine from centers in the midbrain, and dopamine receptors transmit signals over long distance pathways to the frontal cortex, the basal ganglia, and the cerebellum, as shown in the figure on the left. Dopamine is a crucial hormone that orchestrates the brain's thought processes involved in maintaining attention to a task and subsequently acquiring new knowledge. Defective dopamine utilization is widely suspected to play a role in ADHD [36]. Poor quality white matter on these long-distance connections, as a consequence of insufficient supply of fat from the blood, would have a huge impact on the ability to pay attention and to learn new facts. 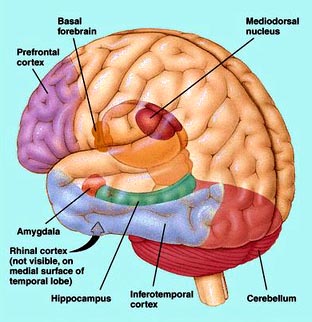 A very exciting research direction that has been undertaken recently addresses the question of the rate of maturation of the brain [31]. 223 children with ADHD were compared with 223 non-ADHD controls. The research utilized magnetic resonance scans to estimate the thickness of the cerebral cortex at more than 40,000 sample points at different positions along the brain surface. Typically, the thickness increases during childhood and then decreases during adolescence. From samples taken over a period of several years, researchers can pinpoint the point in time when the cortex is thickest. The results of the experiments were remarkable: children with ADHD reached peak thickness much later (on average at 10 and a half years old) than children without ADHD (on average at 7 and a half years old). The biggest delay showed up in regions of the prefrontal cortex (shown in the figure on the right) that control attention and motor planning.
A very exciting research direction that has been undertaken recently addresses the question of the rate of maturation of the brain [31]. 223 children with ADHD were compared with 223 non-ADHD controls. The research utilized magnetic resonance scans to estimate the thickness of the cerebral cortex at more than 40,000 sample points at different positions along the brain surface. Typically, the thickness increases during childhood and then decreases during adolescence. From samples taken over a period of several years, researchers can pinpoint the point in time when the cortex is thickest. The results of the experiments were remarkable: children with ADHD reached peak thickness much later (on average at 10 and a half years old) than children without ADHD (on average at 7 and a half years old). The biggest delay showed up in regions of the prefrontal cortex (shown in the figure on the right) that control attention and motor planning.  actually help them think. One way random movements could be effective is through activating dopamine release. Dopamine plays a critical role in body movement: people with Parkinson's disease are unable to initiate movement and appear paralyzed unless treated with the dopamine precursor, L-dopa. I hypothesize that, through random movements of their limbs, ADHD children are able to stimulate the release of dopamine, and thus increase its bioavailability for the important other roles involved in attention and learning.
actually help them think. One way random movements could be effective is through activating dopamine release. Dopamine plays a critical role in body movement: people with Parkinson's disease are unable to initiate movement and appear paralyzed unless treated with the dopamine precursor, L-dopa. I hypothesize that, through random movements of their limbs, ADHD children are able to stimulate the release of dopamine, and thus increase its bioavailability for the important other roles involved in attention and learning.  drug, Ritalin is a very close cousin to amphetamines and exhibitis all of the same dangerous properties leading to addiction and abuse. He cites a 1998 study [18] which showed that the use of a childhood stimulant such as Ritalin "is significantly and pervasively implicated in the uptake of regular smoking, in daily smoking in adulthood, in cocaine dependence, and in lifetime use of cocaine and stimulants."
drug, Ritalin is a very close cousin to amphetamines and exhibitis all of the same dangerous properties leading to addiction and abuse. He cites a 1998 study [18] which showed that the use of a childhood stimulant such as Ritalin "is significantly and pervasively implicated in the uptake of regular smoking, in daily smoking in adulthood, in cocaine dependence, and in lifetime use of cocaine and stimulants."